If you suffer from sebaceous hyperplasia, it can feel like your skin is out of control. Hormonal fluctuations and other factors can cause oil-producing glands to become overactive, resulting in a host of problems like acne, blackheads and whiteheads, and even redness and swelling. But what if we told you that there’s a treatment for your problem that doesn’t involve any drugs or invasive surgery?
The CO2 laser is the perfect solution for treating sebaceous hyperplasia—a technique that uses a beam of light to vaporize small sections of the skin, leaving it free from sebum. This treatment has been shown to be effective in improving the appearance of enlarged pores and reducing the appearance of blackheads and whiteheads. In fact, one study found that more than 80 percent of patients who had undergone CO2 laser treatment reported improvements after just two weeks’ time!
So stop struggling with your skin—and start celebrating all the benefits CO2 lasers have to offer.

CO2 Laser for Sebaceous Hyperplasia
Sebaceous hyperplasia is a common, benign condition of the sebaceous glands. It represents benign enlargement of the sebaceous lobule and around a follicular infundibulum. Lesions are benign with no known potential for malignant transformation and do not require treatment. However, lesions commonly can be cosmetically disturbing and are of aesthetic concern. Treatments are mostly mechanical and tend to recur unless the entire unit is destroyed or excised.
Risk of permanent scarring must be considered when treating benign lesions. Patients often request removal, which may be accomplished by using a wide range of destructive techniques. Unfortunately, treatments for these lesions often result in a depressed scar or are followed by recurrence.
Carbon dioxide lasers have been in use for many years to treat different benign and malignant skin conditions. The ability to rejuvenate sun-damaged, wrinkled skin also has been revolutionized by this technology. For the purpose of destroying sebaceous hyperplasia while also giving the aged face a youthful appearance, our method combines electrodessication and carbon dioxide laser resurfacing.
New Treatment for Sebaceous Hyperplasia
Pathophysiology
Sebaceous glands are present throughout the skin except on the palms and soles. They exist as a component of the pilosebaceous unit or less frequently open directly to the epithelial surface in areas of modified skin. The largest sebaceous glands and the greatest number of sebaceous glands are found on the face, chest, back and upper arms. Sebaceous glands are highly androgen-sensitive and, although the number of sebaceous glands remains approximately the same throughout life, their activity and size vary according to age and circulating hormone levels.
The sebaceous and sweat glands account for the vast majority of androgen metabolism in the skin. At puberty, sebaceous glands enlarge and become increasingly active due to increased production of androgens, and they reach their maximum by the third decade of life. As androgen levels decrease with advancing age, the sebocyte turnover begins to slow down. This decrease in cellular turnover results in crowding of primitive sebocytes, causing a benign hamartomatous enlargement of the sebaceous gland, or sebaceous hyperplasia. This is particularly apparent in the areas where sebaceous glands are concentrated, such as the face. The hyperplastic glands are often inflated up to 10 times their normal size; however, they secrete very little sebum.
Clinical Features
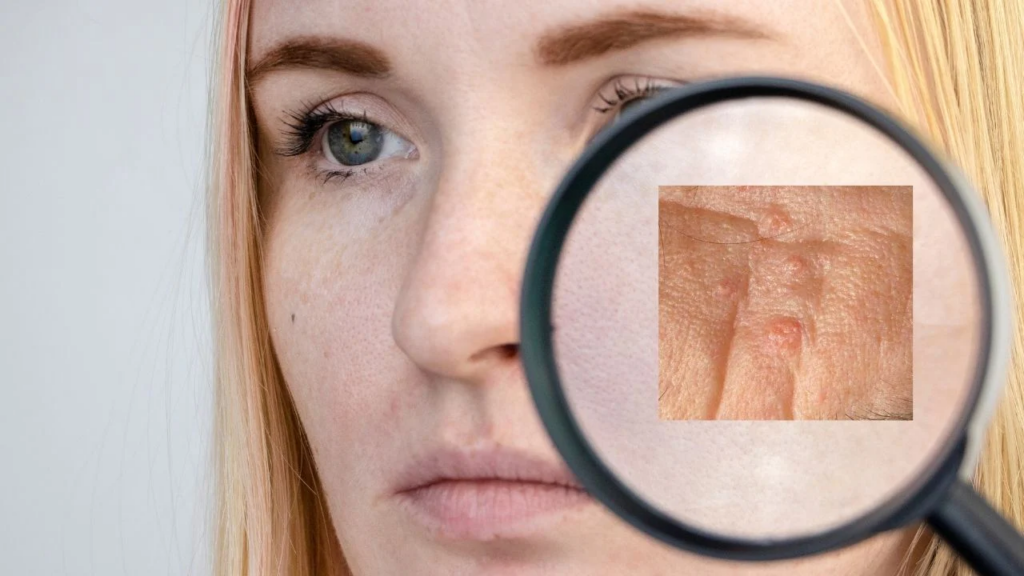
Sebaceous hyperplasia is relatively common in adults of middle age or older. Lesions can present as single or multiple yellowish, occasionally telangiectatic 2-mm to 4-mm papules commonly on the central or upper face and occasionally on the upper trunk, often with central umbilication representing the site of a ductal opening (Figures 1 and 2). Biopsy is occasionally indicated to exclude basal cell carcinoma.
Treatment Options
A variety of treatment options for sebaceous hyperplasia have been described, including topical chemical treatments with bichloracetic or trichloroacetic acid, cauterization or electrodessication, curettage with electrodessication, carbon dioxide laser surgery, cryosurgery, photodynamic therapy, shave excision and oral isotretinoin. Unfortunately, treatment of these lesions often results in a depressed scar or is followed by recurrence.
Patient Selection
Absolute contraindications to carbon dioxide resurfacing include active bacterial, viral or fungal infections. Patient selection is crucial. It is always necessary to review the patient’s expectations and to select patients with realistic expectations as the reason for the procedure is centered on the patient’s desire for the correction and his/her willingness to accept the risks and responsibilities that come with the treatment.
People who have taken oral isotretinoin in the last six months, had a reticular dermis-level resurfacing procedure in the last two to three months, do not want to risk getting redness or lightening after surgery, have collagen vascular disease, Fitzpatrick skin phototypes V and VI, or are likely to get keloid or hypertrophic scars should not have this procedure done. A history of frequent HSV outbreaks is another relative contraindication. Prophylaxis with valacyclovir is given for 10 days even to patients without a history of HSV due to severe consequences should an outbreak occur.
The Procedure
Conscious Sedation We use mild-to-moderate conscious sedation for anesthesia. There is a food and liquid restriction after midnight the night prior to the procedure. Once medical clearance has been obtained, intravenous sedation, similar to “twilight sleep” may be given to eliminate any potential discomfort during the procedure. This will create insensibility or memory to pain without loss of consciousness. Recovery is speedy with twilight anesthesia; usually the side effects associated with general anesthesia, such as vomiting, nausea or dizziness, do not occur.
Patients under conscious sedation still have to be carefully monitored to ensure that they don’t slip into deeper sedation. Electrodessication Electrodessication (Hyfrecator electrosurgical unit) is performed with a sharp noninsulated epilating needle, monoterminal, high-voltage set at 1.5 W. With continuous pressure, the needle is inserted into each lobule, one by one, and desiccated for less than 1 second, resulting in a crackling or popping sound. Resurfacing Following electrodessication, protective eye shields are applied to the patient’s eyes and UltraPulse carbon dioxide laser with CPG scanner for full-facial resurfacing is performed. Our parameters used are 250 mJ, 60 microsecond pulse duration at CPG settings of pattern 29 (rhomboid) at a density of 6.
Laser resurfacing should be performed in a systematic fashion. Resurfacing of a single area alone generally is not advised to avoid sharp demarcations. The scanner allows for rapid, uniform laserbrasion. Clinical advantages include lack of bleeding, markedly shortened time of dissection, and excellent wound healing. In general, as depth of penetration increases, risk of textural changes, scarring and permanent hypopigmentation or depigmentation increases. The safety endpoint is the appearance of a yellow skin color that persists after wiping with saline-soaked gauze, even if the treated lesion persists.
Post Procedure
Patients can expect moderate facial swelling and erythema for 7 to 10 days until healing is complete. Limitations include exercise and makeup during the healing process. Patients may shampoo and rinse their faces 72 hours post procedure, but they should avoid facial cleansing with soap until healing is complete. The continual use of occlusive ointment to prevent crusting and scabbing post procedure will shorten healing time. complications of these destructive therapies include atrophic scarring or transient dyspigmentation.
Sebaceous Hyperplasia Treatment
Sebaceous hyperplasia is a common, benign condition of sebaceous glands. It represents benign enlargement of the sebaceous lobule and around a follicular infundibulum. Lesions are benign with no known potential for malignant transformation and do not require treatment. However, lesions commonly can be cosmetically disturbing and are of aesthetic concern. Treatments are mostly mechanical and tend to recur unless the entire unit is destroyed or excised. Risk of permanent scarring must be considered when treating benign lesions. Patients often request removal, which may be accomplished by using a wide range of destructive techniques.
Unfortunately, treatments for these lesions often result in a depressed scar or are followed by recurrence. Carbon dioxide lasers have been in use for many years to treat different benign and malignant skin conditions. The ability to rejuvenate sun-damaged, wrinkled skin also has been revolutionized by this technology. Our method combines electrodessication followed by carbon dioxide laser resurfacing for sebaceous hyperplasia destruction while at the same time restoring a youthful look to the aged face.
